Age-Related Macular Degeneration (AMD)
Healthful Vitality | 04/11/2019 | By Dr. Sharoon David | Age-Related Macular Degeneration (AMD)
Age-related macular degeneration (AMD) is a retinal pathology that affects the macula lutea, an oval-shaped pigmented area located close to the center of the retina of the eye. The macula is responsible for the high-resolution, central, color vision and accounts for approximately 10% of the entire visual field [1]. AMD damages the macula and leads to a progressive loss of central vision due to degeneration of the photoreceptor-retinal pigment epithelium (RPE) complex.
AMD is considered as one of the leading causes of blindness in the developed countries, where it affects 10% of people who are older than 65 years and over 25% of people who are older than 75 years. Around 2 million individuals in the U.S. have advanced form of AMD and more than 8 million individuals suffer from intermediate disease. A 50% rise in these numbers is expected in the year 2020 [2].
AMD is classified into two major types: the dry type, also known as atrophic or nonexudative type, is more prevalent and involves slow progressive retinal dysfunction. It may eventually develop into the wet or exudative type that is characterized by the formation of abnormal, fragile, and leaky blood vessels (choroidal neovascularization) with subretinal or intraretinal hemorrhage, leakage, or retinal pigment epithelial detachment [3].
Etiology
The etiology of age-related macular degeneration (AMD) is multifactorial and is associated with genetic as well as environmental risk factors. Older age, family history, cigarette smoking, higher body mass index (BMI), hyperlipidemia, hypertension, history of cardiovascular disease, and light iris color are some of the proposed risk factors for AMD [2, 4].
Advancing age is considered to be the strongest risk factor for the development of AMD. AMD has been found to be infrequent in individuals who are under 50 years of age, and in comparison, to patients between the ages of 65 to 74 years, those who are over 75 years of age have a threefold greater risk of acquiring AMD [2].
A positive history of AMD in a first-degree relative greatly increases the likelihood of developing this condition. Siblings of an AMD patient have been found to have a three to six times greater risk as compared to siblings of healthy individuals [2, 5].
Cigarette smoking is a proven modifiable risk factor for not only the development and progression of AMD but also for the clinical response in both forms of AMD. By promoting molecular and pathological changes, smoking may establish a macular microenvironment that is ideal for the development of AMD [6]. Individuals who smoke cigarettes for more than 40 years have a two to four times higher risk for developing AMD as compared to nonsmokers of the same age [2].
Pathogenesis
The exact pathogenesis of AMD is yet not fully understood; however, it is believed to involve complex pathological mechanisms at cellular, molecular, and biochemical levels [7].
With advancing age, lipofuscin containing intracellular residual bodies accumulate in the retinal pigment epithelium (RPE) cells. These materials are normally expressed by the RPE cells and are transported across the Bruch’s membrane (BM) to be eliminated by the choroidal blood vessels. Bruch’s membrane (BM) is the innermost layer of the choroid and separates the RPE from the choriocapillaries. Thickening of the BM is an early defect seen in AMD. This leads to alterations in the permeability of the BM, and thus the extruded waste material gets accumulated between the RPE and the BM in the form of focal deposits, known as drusen, which are considered to be the hallmark of early AMD [2, 7].
Drusen formation indicates RPE dysfunction, which promotes RPE and photoreceptor loss. Further RPE degeneration can result in dysfunction of the BM. Progressive breakdown of the BM and the upregulation of vascular endothelial growth factor (VEGF) may promote choroidal neovascularization (CNV), a process involving the growth of abnormal choroidal vessels under the RPE and, potentially, beneath the retina. These abnormal vessels may leak and bleed before regressing and forming a disciform scar. A permanent loss of central vision is, therefore, the end-stage of exudative AMD [2, 8].
Clinical Features
Age-related macular degeneration (AMD) may affect one or both the eyes. The recognition of symptoms suspicious of AMD is important in alerting the clinician to refer the patient to a specialist for a comprehensive assessment. The symptoms of AMD may include [9, 10, 11]:
- Progressive or sudden decrease in vision that is not improved with optic correction
- Blurring, distortion, or darkening of the central part of the visual field
- Metamorphopsia (Distortion of visual images) – The patient may see straight lines as wavy or crooked. This is a hallmark sign seen in patients with macular disorders
- Micropsia (objects appear smaller than normal) or macropsia (objects seem larger than normal)
- Loss of central vision may interfere with everyday activities, such as recognizing faces, reading, writing, watching television, going around a corner, and driving
Diagnosis
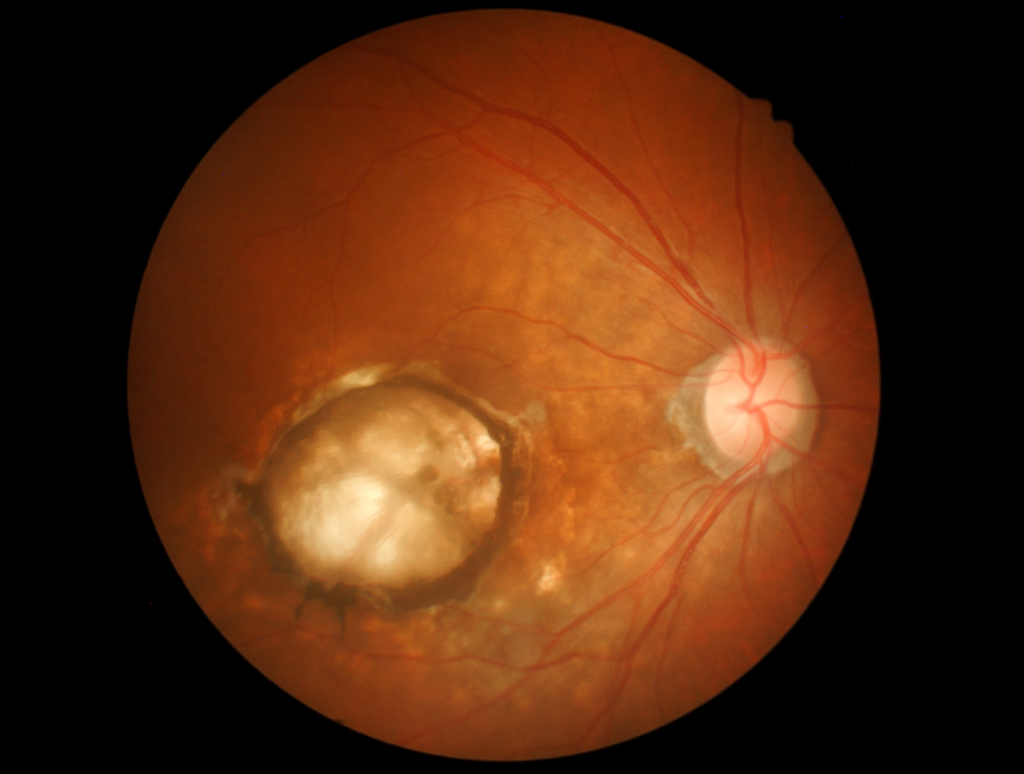
Dry AMD is characterized by variable sizes, types, and distribution of drusen at the posterior pole. Pigmentary disturbances are frequently seen and may be in the form of focal hypopigmentation or hyperpigmentation. Atrophy of the RPE may be visible in the form of progressive well-demarcated patches in the perifoveal area. With time, these patches may enlarge and coalesce, resulting in geographic atrophy (GA). The features of wet AMD may include drusen, pigment epithelial detachment (PED), choroidal neovascularization, and intraretinal or subretinal hemorrhage or fluid [2].
A dilated examination of the fundus is essential for the correct diagnosis of AMD [9]. In addition to this, several imaging studies are also performed [2, 10, 12, 13]:
Optical coherence tomography (OCT)
It is helpful in diagnosing early AMD. Drusen may be seen as elevations at the RPE level. OCT may also be used to determine the presence of intraretinal or subretinal blood or fluid in exudative AMD.
Digital fundus photography
It may be effective in documenting clinical findings in both dry and wet AMD. However, media clarity, fundus pigmentation, image quality, noise, resolution, and sensitivity of the camera are some of the difficulties that may hinder the precision of color fundus photograph measurements.
Fundus autofluorescence (FAF) imaging
It is beneficial in the evaluation and monitoring of the health and topographic structure of the RPE. GA may be seen as a well-circumscribed dark area clearly demarcating atrophy of the RPE.
Fluorescein angiography (FA)
It is the gold standard for identifying and confirming the source of choroidal neovascularization (CNV). Angiography can help determine the exact location of the neovascular complex and can assist in guiding treatment with intravitreal injections or laser.
Indocyanine green angiography (ICGA)
It involves the use of the indocyanine green (ICG) dye instead of the fluorescein dye. ICG dye is retained in the choroidal circulation and thus, is useful for the imaging of choroidal circulation. ICGA may be helpful in evaluating specific forms of AMD, e.g., occult CNV.
Treatment
Several therapeutic approaches, including stem-cell therapy, are under investigation for the treatment of dry AMD. However, there is no approved treatment option available currently [14, 15]. The early recognition of visual changes and the detection of choroidal neovascularization at a treatable stage is, therefore, of great significance. An Amsler grid is a chart that can be used by the patients for the monitoring of any changes, such as the presence of scotoma or metamorphopsia, in the central field of vision [9].
Cigarette smoking is strongly associated with AMD. Hence, smoking cessation is an important primary therapeutic recommendation that may help reduce the burden of disease [16, 17]. Moreover, recent research including the AREDS and AREDS2 trials, have demonstrated that the use of a combination of zinc, antioxidant vitamins like vitamin C and E, and carotenoids may have a beneficial role in retarding the progression of disease [14, 15, 18, 19].
Progress in the management of wet AMD
Significant progress has been made in the management of wet AMD in recent years. Intravitreal injection therapy with anti-VEGF agents is being used for the treatment of wet AMD with active choroidal neovascularization. Several anti-VEGF agents are available for this purpose. Ranibizumab, a monoclonal antibody fragment (Fab), is approved by the FDA for the treatment of neovascular AMD. Aflibercept is another FDA-approved anti-VEGF agent that is available for use. Bevacizumab, a monoclonal anti-VEGF-A antibody, is currently approved by the FDA for the treatment of colorectal cancer. However, it has been used by many retina specialists as an off-label medication for the treatment of neovascular AMD [18, 20].
Photodynamic therapy (PDT) may be required in a selected minority of patients who do not respond to anti-VEGF therapy. It involves the intravenous administration of a photosensitizer, verteporfin, which is activated by photons from a low-energy visible red laser. The activated dye results in the formation of reactive-free radicals that induce damage to the vascular endothelium and lead to the occlusion of abnormal new choroidal vessels [18].
Age-related macular degeneration (AMD) is a significant cause of visual morbidity worldwide. Our current understanding regarding the exact pathogenesis of AMD remains imprecise. However, substantial research efforts are in progress in order to improve our understanding of the disease as well as to identify and evaluate new therapeutic modalities for its treatment.
Important points:
- AMD is a retinal pathology that affects the macula
- It is one of the leading causes of blindness worldwide
- It has two major types: dry or nonexudative and wet or exudative
- Advancing age, family history, and cigarette smoking are important risk factors
- It may lead to permanent loss of central vision
- No approved treatment for dry AMD is available at present
- Intravitreal anti-VEGF injections are used to treat wet AMD
References:
- Hageman GS, Gehrs K, Johnson LV, et al. Age-Related Macular Degeneration (AMD) 2008 Jan 1. In: Kolb H, Fernandez E, Nelson R, editors. Webvision: The Organization of the Retina and Visual System [Internet]. Salt Lake City (UT): University of Utah Health Sciences Center; 1995-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK27323/
- Al-Zamil WM, Yassin SA. Recent developments in age-related macular degeneration: a review. Clin Interv Aging. 2017;12:1313-1330. Published 2017 Aug 22. doi:10.2147/CIA.S143508. Available at: https://pubmed.ncbi.nlm.nih.gov/28860733/
- Hernández-Zimbrón LF, Zamora-Alvarado R, Ochoa-De la Paz L, et al. Age-Related Macular Degeneration: New Paradigms for Treatment and Management of AMD. Oxid Med Cell Longev. 2018;2018:8374647. Published 2018 Feb 1. doi:10.1155/2018/8374647. Available at: https://pubmed.ncbi.nlm.nih.gov/29484106/
- Chakravarthy U, Wong TY, Fletcher A, et al. Clinical risk factors for age-related macular degeneration: a systematic review and meta-analysis. BMC Ophthalmol. 2010;10:31. Published 2010 Dec 13. doi:10.1186/1471-2415-10-31. Available at: https://pubmed.ncbi.nlm.nih.gov/21144031/
- Shahid H, Khan JC, Cipriani V, et al. Age-related macular degeneration: the importance of family history as a risk factor. British Journal of Ophthalmology 2012;96:427-431. Available at: https://pubmed.ncbi.nlm.nih.gov/21865200/
- Velilla S, García-Medina JJ, García-Layana A, et al. Smoking and age-related macular degeneration: review and update. J Ophthalmol. 2013;2013:895147. Available at: https://pubmed.ncbi.nlm.nih.gov/24368940/
- Al Gwairi O, Thach L, Zheng W, Osman N, Little PJ. Cellular and Molecular Pathology of Age-Related Macular Degeneration: Potential Role for Proteoglycans. J Ophthalmol. 2016;2016:2913612. Available at: https://pubmed.ncbi.nlm.nih.gov/27563459/
- Biesemeier A, Taubitz T, Julien S, Yoeruek E, Schraermeyer U. Choriocapillaris breakdown precedes retinal degeneration in age-related macular degeneration. Neurobiol Aging. 2014;35: 2562–2573. 10.1016/j.neurobiolaging.2014.05.003. Available at: https://pubmed.ncbi.nlm.nih.gov/24925811/
Also Read: Normal Saline or Balanced Crystalloids?
- García-Layana A, Cabrera-López F, García-Arumí J, Arias-Barquet L, Ruiz-Moreno JM. Early and intermediate age-related macular degeneration: update and clinical review. Clin Interv Aging. 2017;12:1579-1587. Published 2017 Oct 3. doi:10.2147/CIA.S142685. Available at: https://pubmed.ncbi.nlm.nih.gov/29042759/
- National Institute for Health and Care Excellence (UK). Age-related macular degeneration: diagnosis and management. London: National Institute for Health and Care Excellence (UK); 2018 Jan. (NICE guideline, No. 82.) 7, Diagnosis. Available from: https://www.ncbi.nlm.nih.gov/books/NBK536479/
- Informed Health Online [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006-. Age-related macular degeneration (AMD): Overview. 2006 May 22 [Updated 2018 May 3].Available from: https://www.ncbi.nlm.nih.gov/books/NBK315804/
- Ly A, Nivison-Smith L, Zangerl B, Assaad N, Kalloniatis M. Advanced imaging for the diagnosis of age-related macular degeneration: a case vignettes study. Clin Exp Optom. 2017;101(2):243-254. Available at: https://pubmed.ncbi.nlm.nih.gov/28994139/
- Adam J. Gess, Anne E. Fung & Jorge G. Rodriguez (2011) Imaging in Neovascular Age-Related Macular Degeneration, Seminars in Ophthalmology, 26:3, 225-233. https://pubmed.ncbi.nlm.nih.gov/21609236/
- Bandello F, Sacconi R, Querques L, Corbelli E, Cicinelli MV, Querques G. Recent advances in the management of dry age-related macular degeneration: A review. F1000Res. 2017;6:245. Published 2017 Mar 9. doi:10.12688/f1000research.10664.1
Also Read: “Anesthesia-Induced Neurotoxicity in Pediatric Patients” – By Dr. Sharoon David)
- Sacconi R, Corbelli E, Querques L, Bandello F, Querques G. A Review of Current and Future Management of Geographic Atrophy. Ophthalmol Ther. 2017;6(1):69-77. Available at: https://pubmed.ncbi.nlm.nih.gov/28391446/
- Martin L. Targeting modifiable risk factors in age-related macular degeneration in optometric practice in Sweden. Clin Optom (Auckl). 2017;9:77-83. Published 2017 Apr 19. doi:10.2147/OPTO.S129942. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6095576/
- Gopinath B, Flood VM, Kifley A, Liew G, Mitchell P. Smoking, antioxidant supplementation and dietary intakes among older adults with age-related macular degeneration over 10 years. PLoS One. 2015;10(3):e0122548. Published 2015 Mar 30. doi:10.1371/journal.pone.0122548. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4378919/
- Yonekawa Y, Miller JW, Kim IK. Age-Related Macular Degeneration: Advances in Management and Diagnosis. J Clin Med. 2015;4(2):343-59. Published 2015 Feb 12. doi:10.3390/jcm4020343. Available at: https://pubmed.ncbi.nlm.nih.gov/26239130/
- Wright CB, Ambati J. Dry Age-Related Macular Degeneration Pharmacology. Handb Exp Pharmacol. 2017;242:321-336. Available at: https://pubmed.ncbi.nlm.nih.gov/27900609/
- Alexandru MR, Alexandra NM. Wet age related macular degeneration management and follow-up. Rom J Ophthalmol. 2016;60(1):9-13. Available at: https://pubmed.ncbi.nlm.nih.gov/27220225/